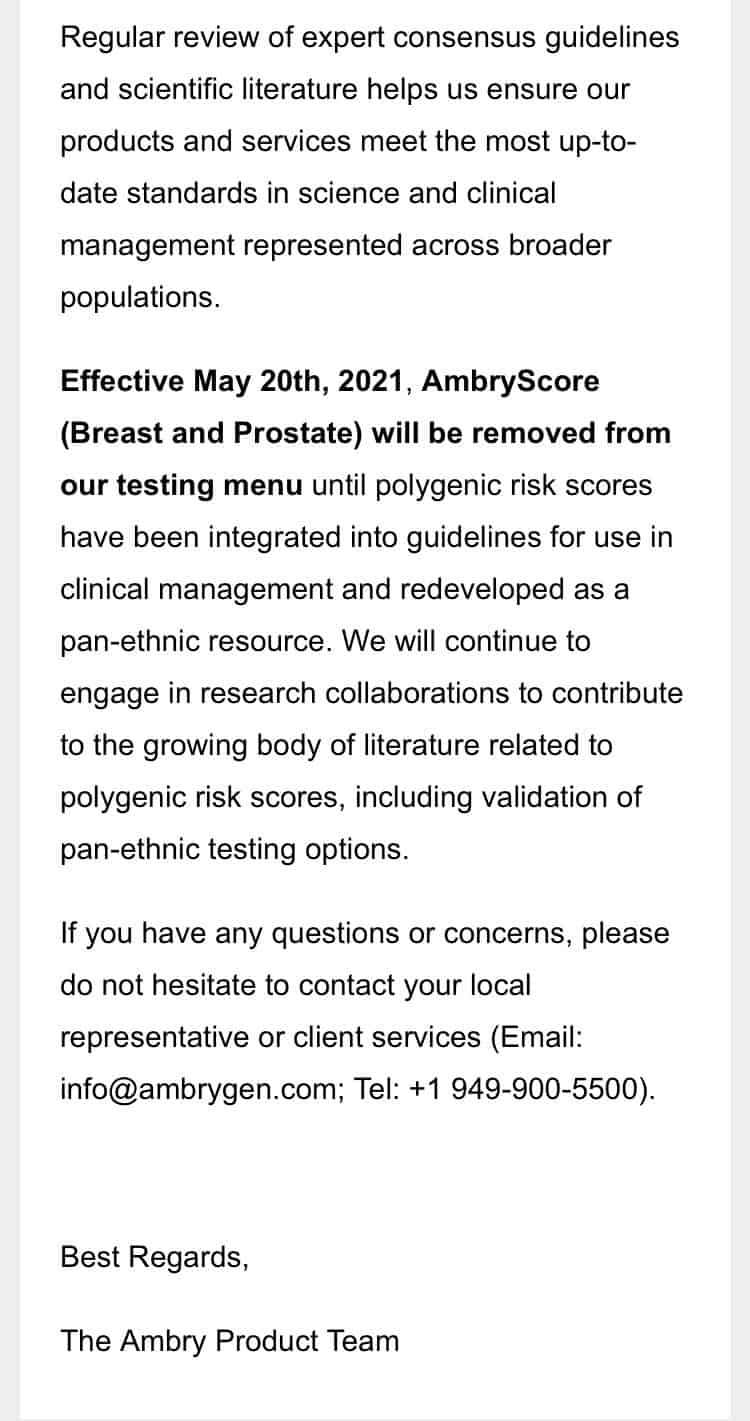
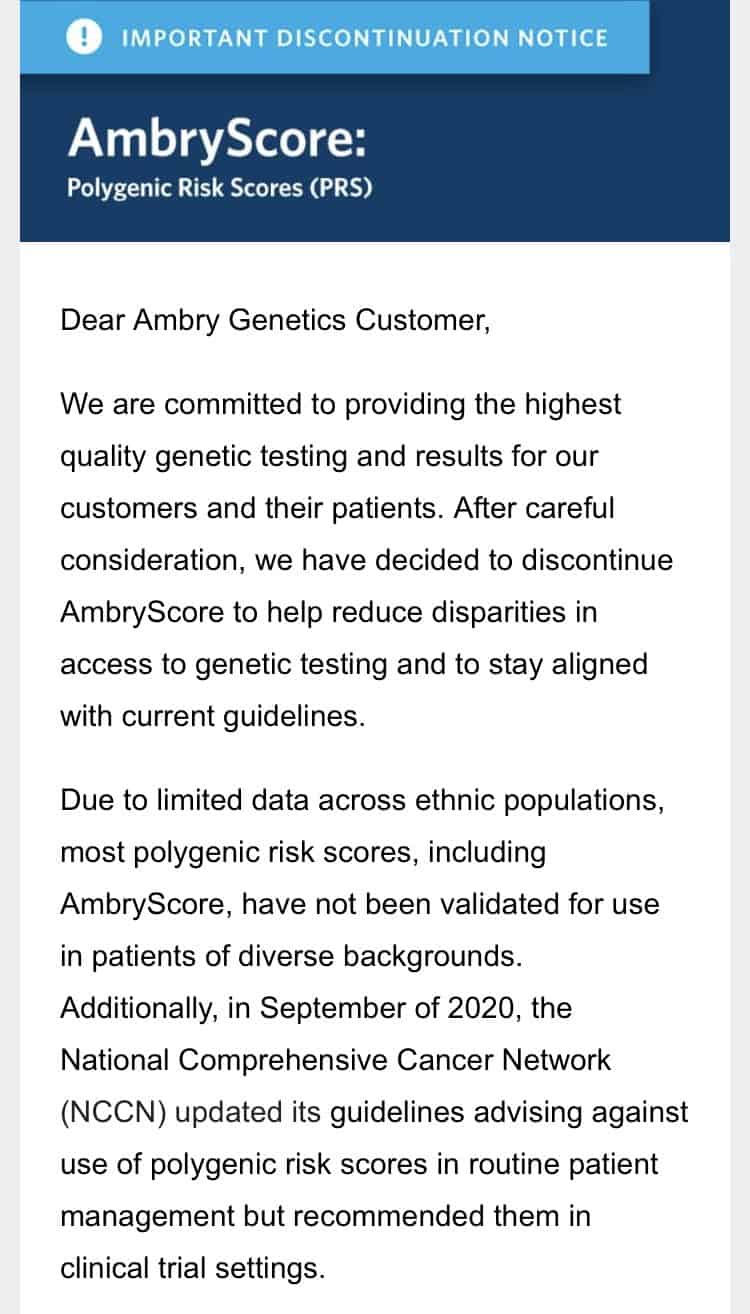
 A few people shared with me some screenshots from a message from Ambry Genetics regarding polygenic risk scores (click to enlarge). From what I can gather this seems to indicate that they’ll stop offering polygenic risk scores until they become more equitable by population. The basic issue here is that a prediction for one population may not port over well to another. The standard “solution” to this problem has been to expand population coverage by doing more research on non-European populations.
A few people shared with me some screenshots from a message from Ambry Genetics regarding polygenic risk scores (click to enlarge). From what I can gather this seems to indicate that they’ll stop offering polygenic risk scores until they become more equitable by population. The basic issue here is that a prediction for one population may not port over well to another. The standard “solution” to this problem has been to expand population coverage by doing more research on non-European populations.
Perhaps I’m misunderstanding, but the communication here seems to suggest that they will stop giving scores to people of European ancestry until they can provide them to other groups in the interests of equity.
The communication here was shared on genetic counselor Twitter, and the messages were all very supportive. Generally, they were of the form “this is how antiracism is done!”
If I understand this correctly, I am not supportive. The traditional means by which these sorts of inequities were remediated is through addition, not subtraction. Not providing a polygenic risk score that might be actionable and useful to white Americans would be like simply rejecting using standardized tests because there is a gap between races.
There are two major issues here. First, “white Americans” are heterogeneous socioeconomically. White American life expectancy is declining. This decline is driven by social and class stratification. A focus on racial equity masks this reality. Due to the interaction of the environment with genetic risk improving equity through subtraction will increase class inequity. The white Americans who could benefit the most from polygenic risk scores because of all their environmental risks are probably Hillbilly Elegy whites.
Second, there has and will be progress in diversifying the training sets with non-Europeans. We can’t get worse than where we are. The issue is not racism in the classical sense, but various structural and historical forces (outside of East Asia most of the studies have been done in the USA and Europe). And, you can’t chalk up all the blame to Americans and Europeans. India and the Middle East in particular have great possibilities in the domain of biomedical genetics due to inbreeding and endogamy but have not leveraged their natural advantage in this area due to bureaucratic inaction and lack of execution. The scientists in these nations want to “go” but the political and institutional support is not there, or slows them down.
I must also add that I have heard privately from some researchers who are white that they have made a private decision to shy away from research on non-Europeans due to the possibility of controversy. Basically, some activists may not believe it is a “good look” for white people to be doing research on datasets of “people of color,” so on a personal level of decision-making, some white scholars are just leaving the work to nonwhite scholars. This is not a good trend in my opinion, though I understand why individuals with really diverse career options would choose the maximum gain for the minimum risk.